Hi,
I tried the multi-tissue CSD pipeline on single shell data with the WM and CSF responses follwed by mtnormalize (response functions and fod results enclosed).
Can the experts/other users confirm if they look ok 
Best,
Karthik
Hi,
I tried the multi-tissue CSD pipeline on single shell data with the WM and CSF responses follwed by mtnormalize (response functions and fod results enclosed).
Can the experts/other users confirm if they look ok
Best,
Karthik
Hi again @Kar,
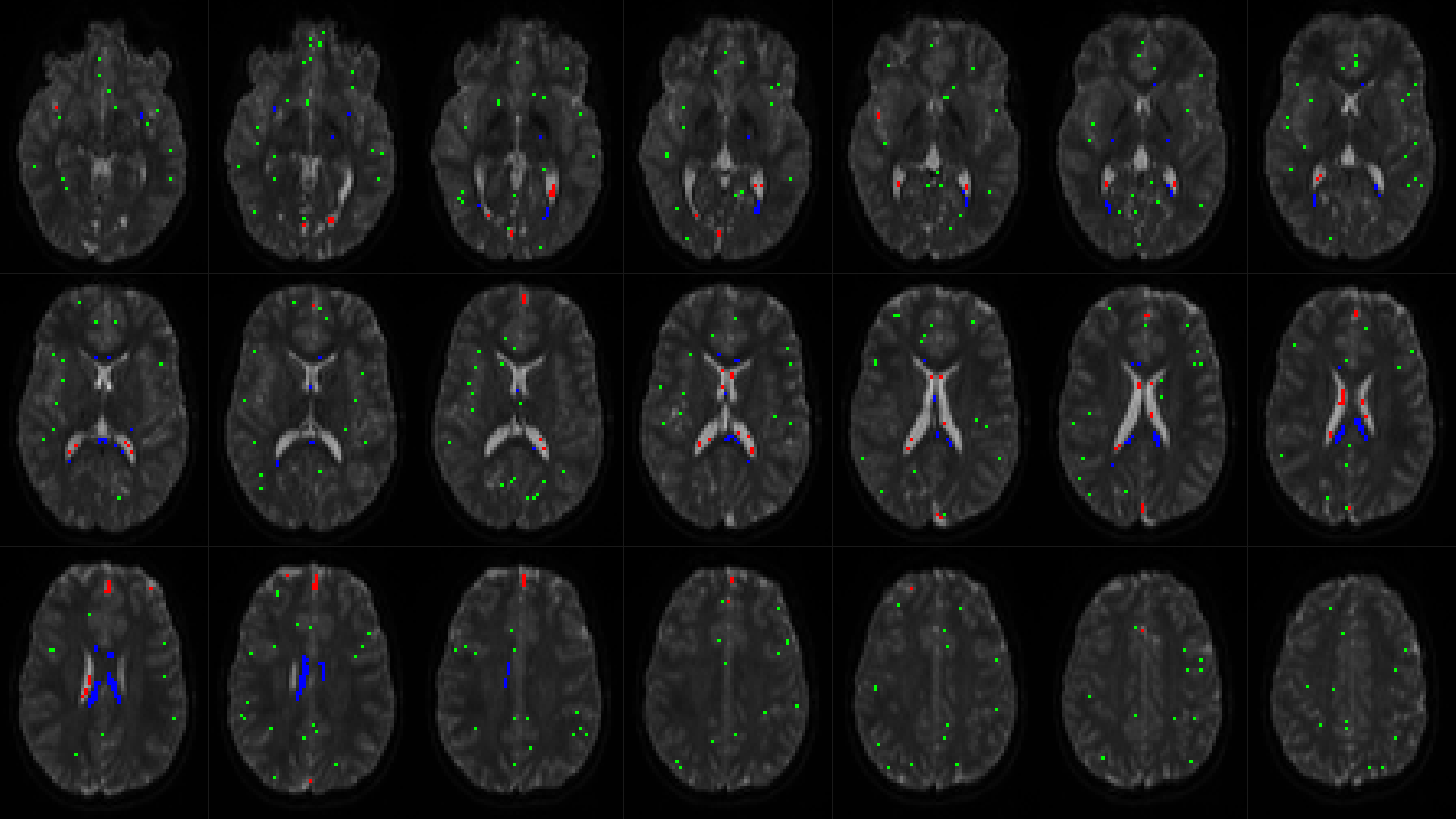
Looks generally ok. The only risk/concern in this case, which I can’t tell immediately from these images only, would be that your CSF response comes from an area that is “too generous”. You can confirm whether this is the case (or not) by looking at the -voxels output of dwi2response dhollander, and overlaying it on any of your images for reference. To do this, open any of your images (e.g. your actual “CSF” image you’ve shown above) in mrview, and open the voxel.mif (or whatever you named it) in the overlay tool. Next, in the overlay tool, switch “interpolation” off (at the bottom of the tool) and add a lower threshold of a value smaller than 1 (e.g. 0.1 or 0.5 or whatever  ). Then going to e.g. lightbox mode, you can generate a view that looks something like this:
). Then going to e.g. lightbox mode, you can generate a view that looks something like this:
This gives you/us a good idea of what voxels where exactly selected, so you can confirm if things make sense. Even though you’re only after WM-CSF CSD, it’s still quite a valuable quality-check to even pay close attention to the selected “GM” voxels (see my email). Working with rodent data, or for other people that may be working with ex-vivo data, or other funny/challenging scenarios, it may be worthwhile playing around with the -fa parameter to dwi2response dhollander. In any more “normal” scenario, this should never be needed. But in any “special” scenario, this may make the difference between things seemingly refusing to work and suddenly magically working out. In most of those “special” scenarios, the change to -fa you’d be looking for, is lowering its default value of 0.2 to e.g. 0.1. See again my email for details.
If you’re keen to share, feel free to post a few extra screenshots showing the voxel selection!
Cheers,
Thijs
For completeness sake: the above example was overlaid on an (average, if I recall correctly) b=0 image of the subject. That’s typically good enough for anatomical reference.
Hi Thijs,
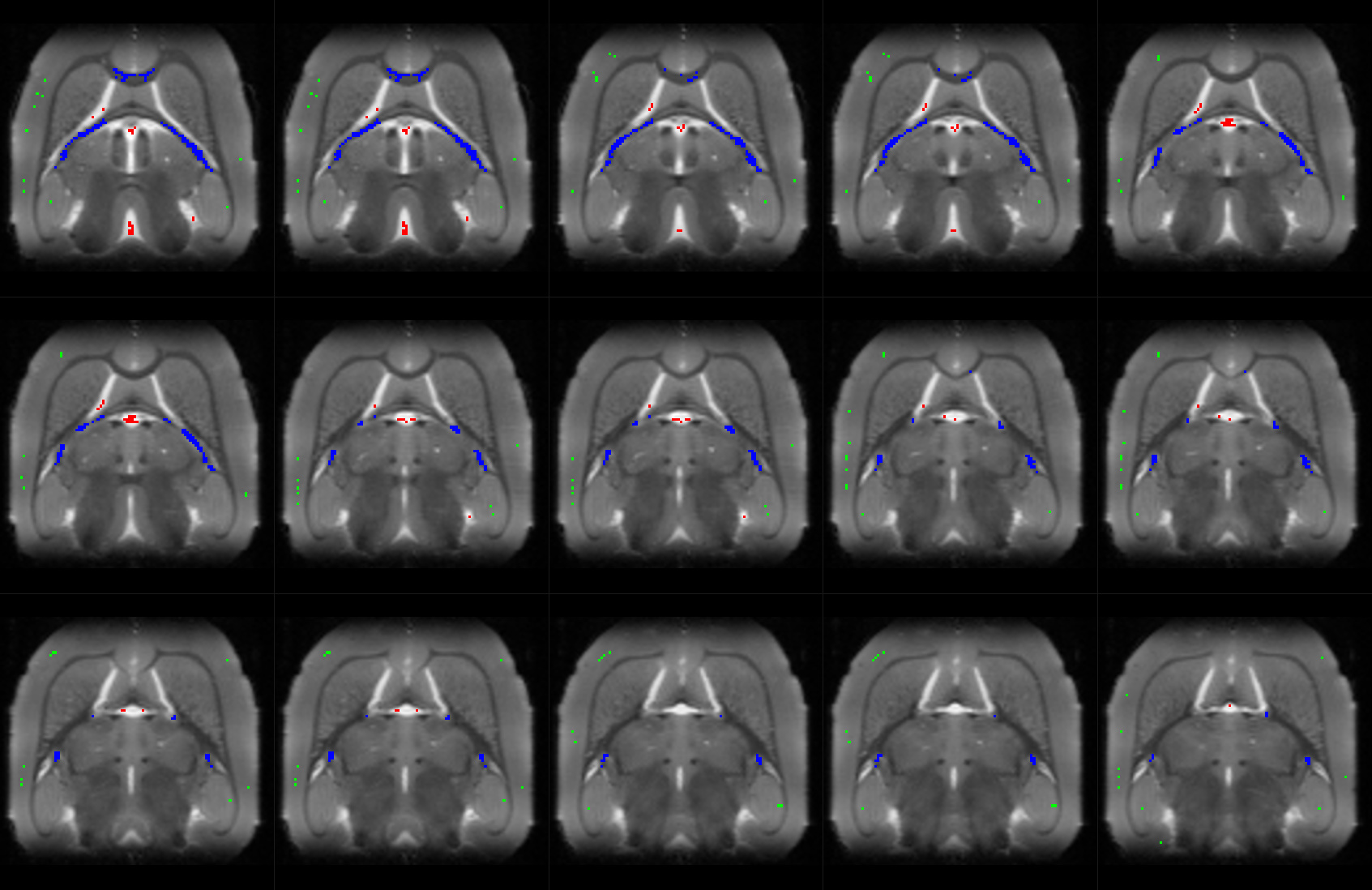
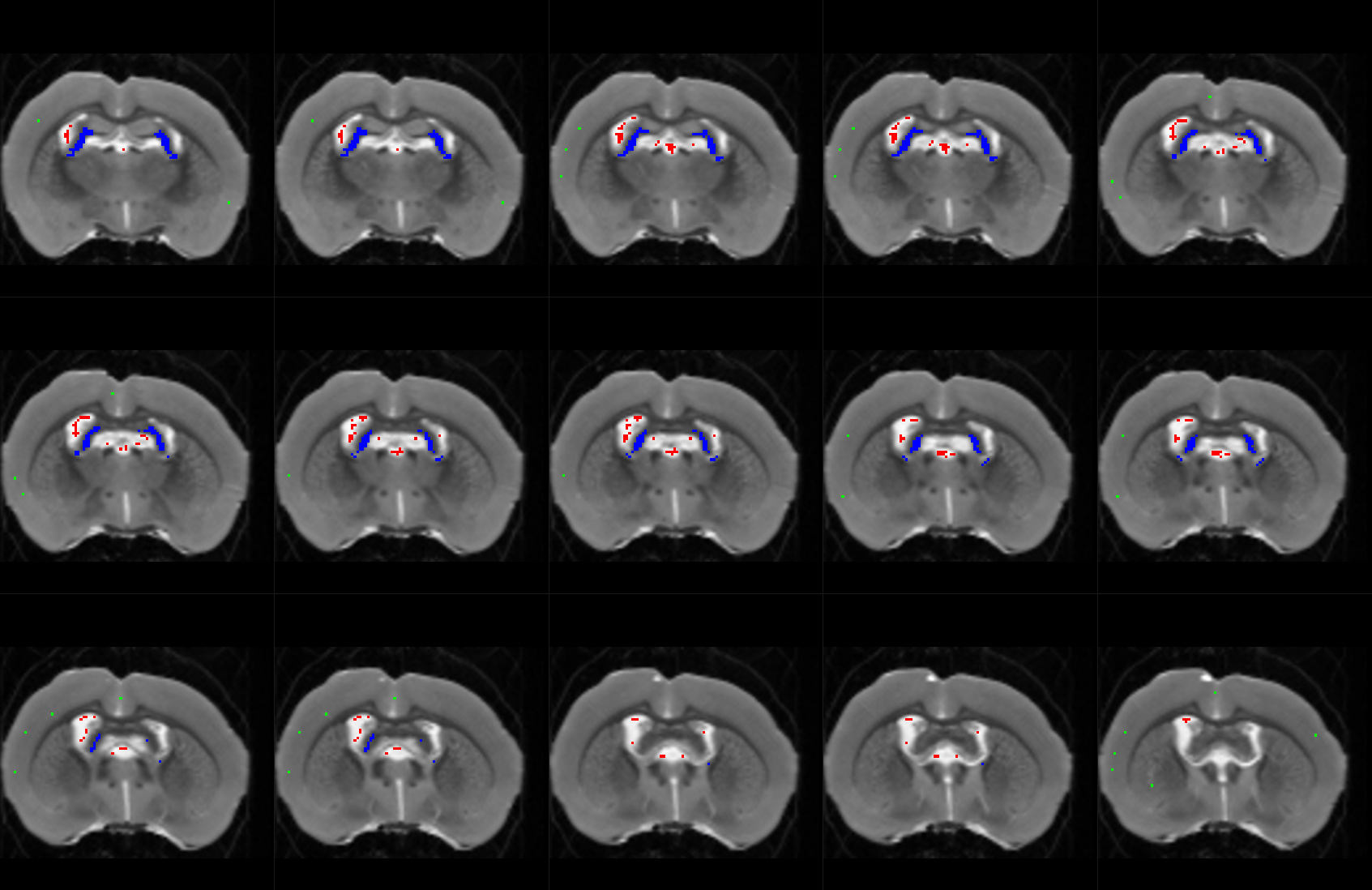
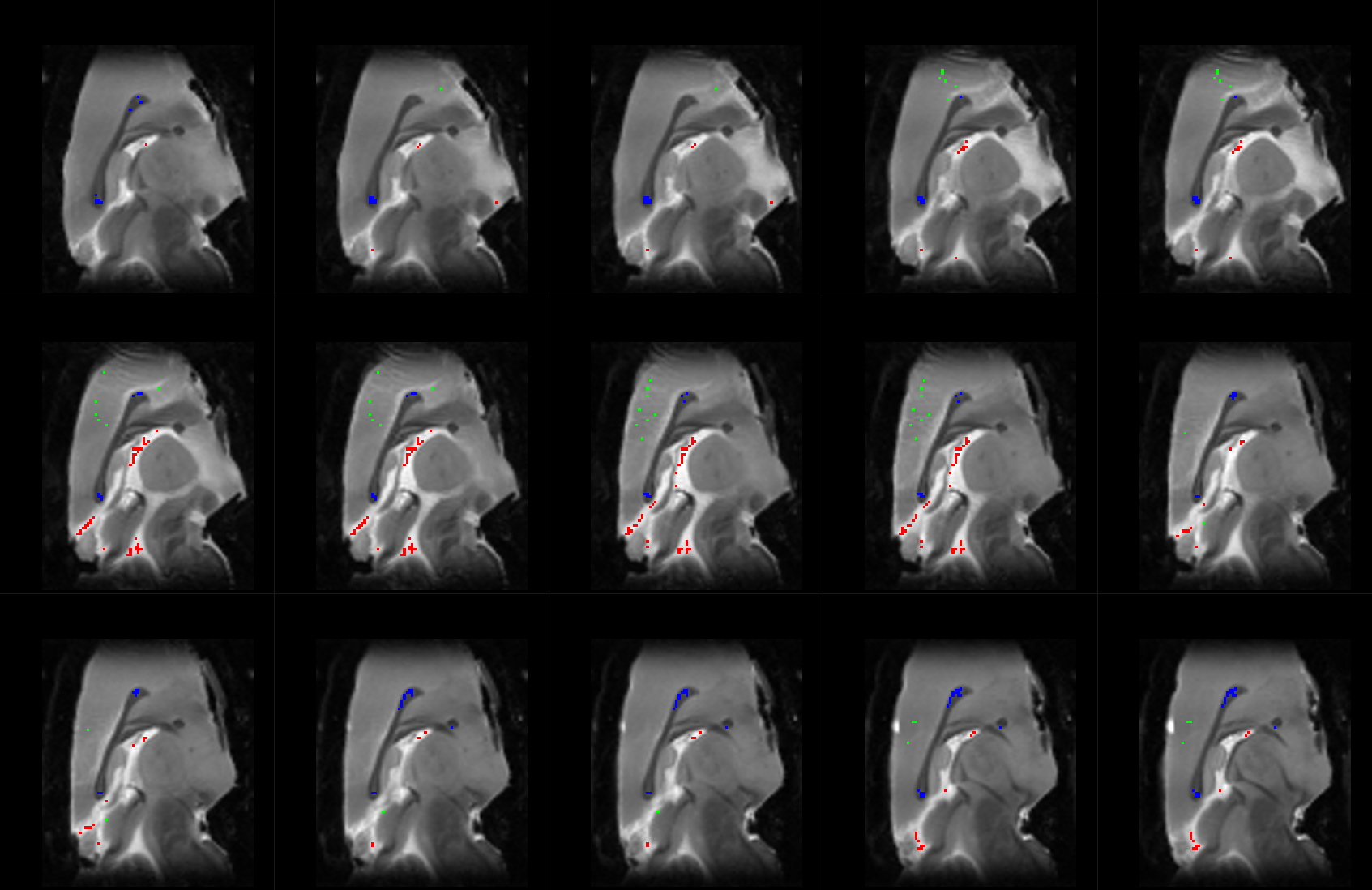
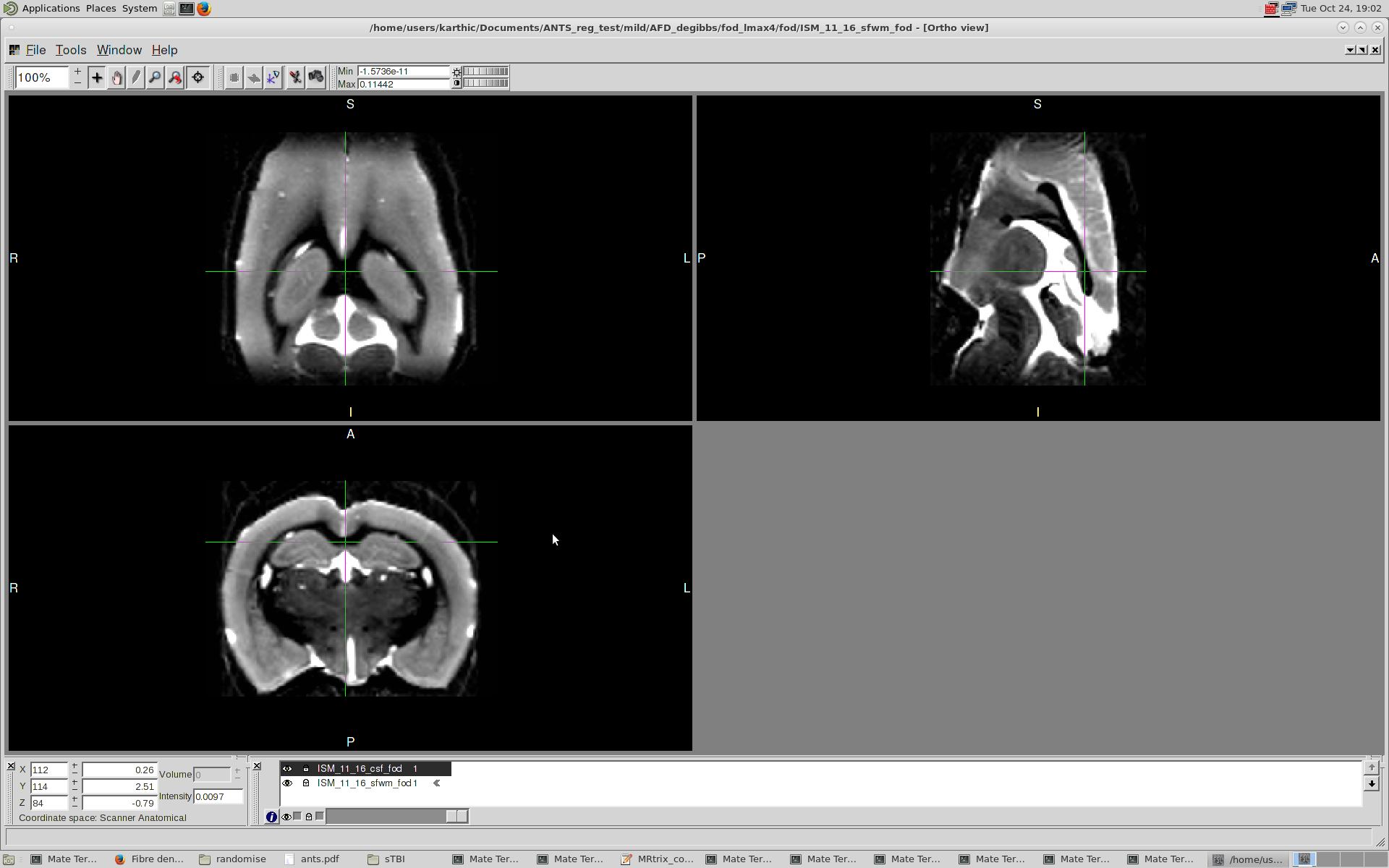
I’m getting back to you with results from the voxel selection overlaid on the B0 images (after lowering the threshold to 0.1).
They seem pretty neat to me! Looking forward to your comments
Best,
Karthik
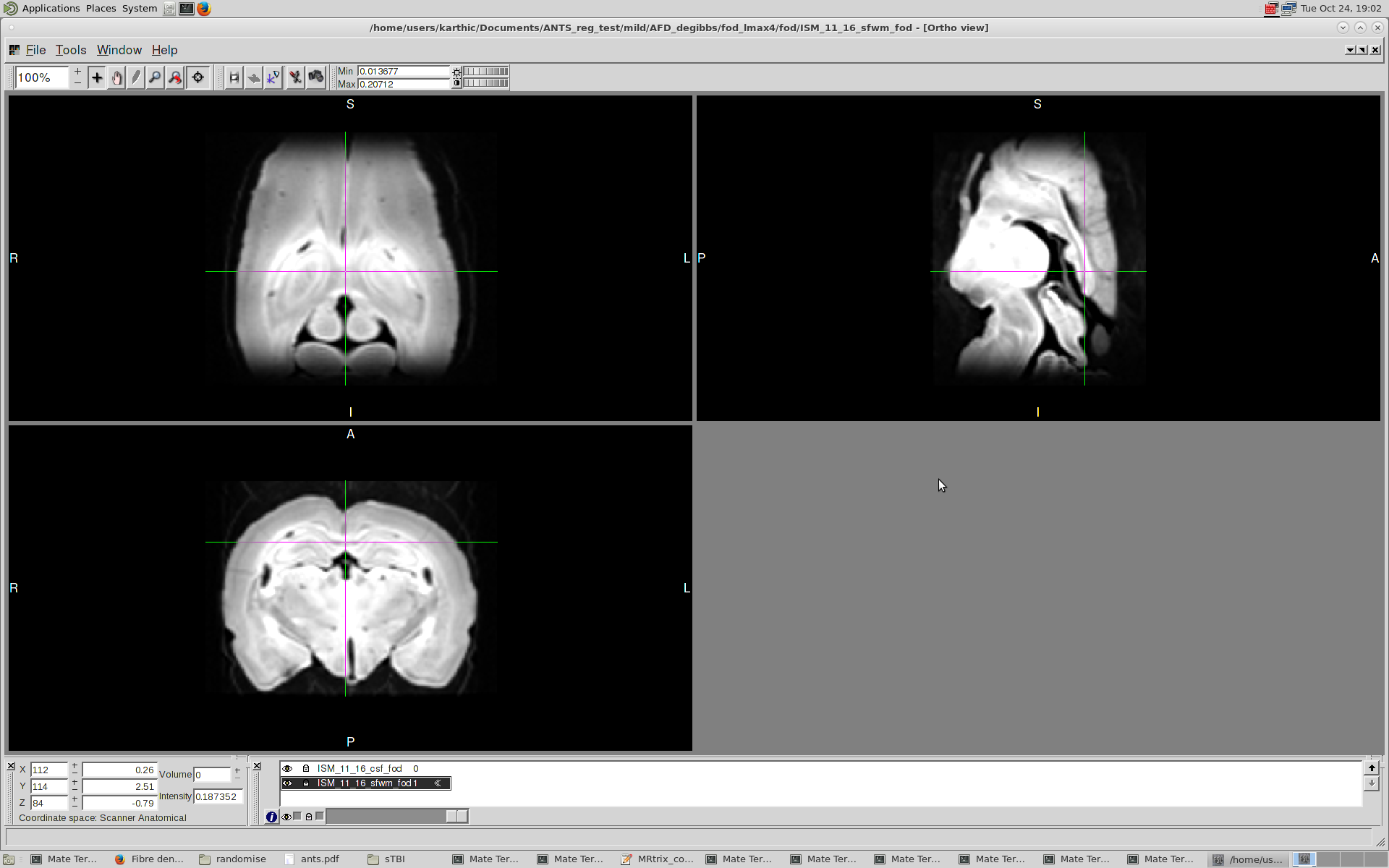
![]() Absolutely beautiful! These should do the job. It would be interesting to see if the 2-tissue WM-CSF CSD result is any different. There’s a possibility it’s actually very similar, but then again also another possibility that this change to the response functions made an important difference. I’m starting to come round more and more to the fact that the
Absolutely beautiful! These should do the job. It would be interesting to see if the 2-tissue WM-CSF CSD result is any different. There’s a possibility it’s actually very similar, but then again also another possibility that this change to the response functions made an important difference. I’m starting to come round more and more to the fact that the dwi2response dhollander is even much more robust than I’d initially anticipated when I designed it. I used to say that it was only guaranteed to work decently on developed (> 3yo) in vivo human data of healthy subjects, but recently more and more of those limitations in that statement have been shown to be inherently overcome by the algorithm. Depending on the scenario though, the -fa parameter may indeed require slight tweaking. But once setting it right for a given application, it again applies across the board.
What I’d personally do in your case, i.e. studying a TBI model versus control group, is estimate the response functions in this way for all your control animals, and then averaging them per tissue type, as described in the multi-tissue FBA manual. Depending on the extent of the damage present in the TBI model, the response functions you’d get from those TBI animals may not necessarily be the best model of healthy tissue. Performing n-tissue CSD, the response functions are the units/model that describes and hence decides the interpretation of the outcome. With this in mind, it’s probably wise to choose the response functions to reflect tissue signals that are better understood/described/…, i.e. healthy tissue classes. Expressing pathology in function of healthy tissue signals may very well provide the most intuitive handle on pathology you can get using n-tissue CSD. I wouldn’t be surprised to see an increase in CSF-like signals in regions affected by severe TBI effects, given enough time after the original impact damage, using 2-tissue WM-CSF CSD.
Cheers,
Thijs
Thanks for the suggestions!! I have started processing the data with just the control group response functions 
I will keep you posted as and when I get some issues & hopefully, interesting results 
Regards,
Karthik
Sounds great! Let’s hope things work out well.